1801006062-LONG CASE
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of “ patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
LONG CASE :
CHIEF COMPLAINTS:
A 40 year old female resident of suryapet came to the OPD with chief complaints of generalised weakness and generalised body pains and unable to walk since 6 months
HISTORY OF PRESENT ILLNESS :
Patient is apparently asymptomatic 3 years ago then in 2019 she developed weakness in left lower limb which is sudden in onset and gradually progressive for which she consulted a local doctor and found to have low levels of potassium and have been supplemented with potassium then the attack was subsided.
Sequence of illness after the first episode :
In November 2021 :
History of severe episode of upper limb and lower limb weakness , loss of consciousness for 2 days and loss of speech for 2 days and she also has history of decreased bowel movements and again diagnosed as hypokalaemia and treated with potassium supplements and kept on ventilation and blood transfusion (1 unit ) is done and discharged after 5 days
on may 2022 :
She has similar complaints as past but which is less severe and she is able to walk and she is conscious and again treated for hypokalaemia and discharged in 3 days
February 2023 :
Similar complaints as past and presented with 2 episodes of vomitings which are non bilious , non projectile and food particles as content
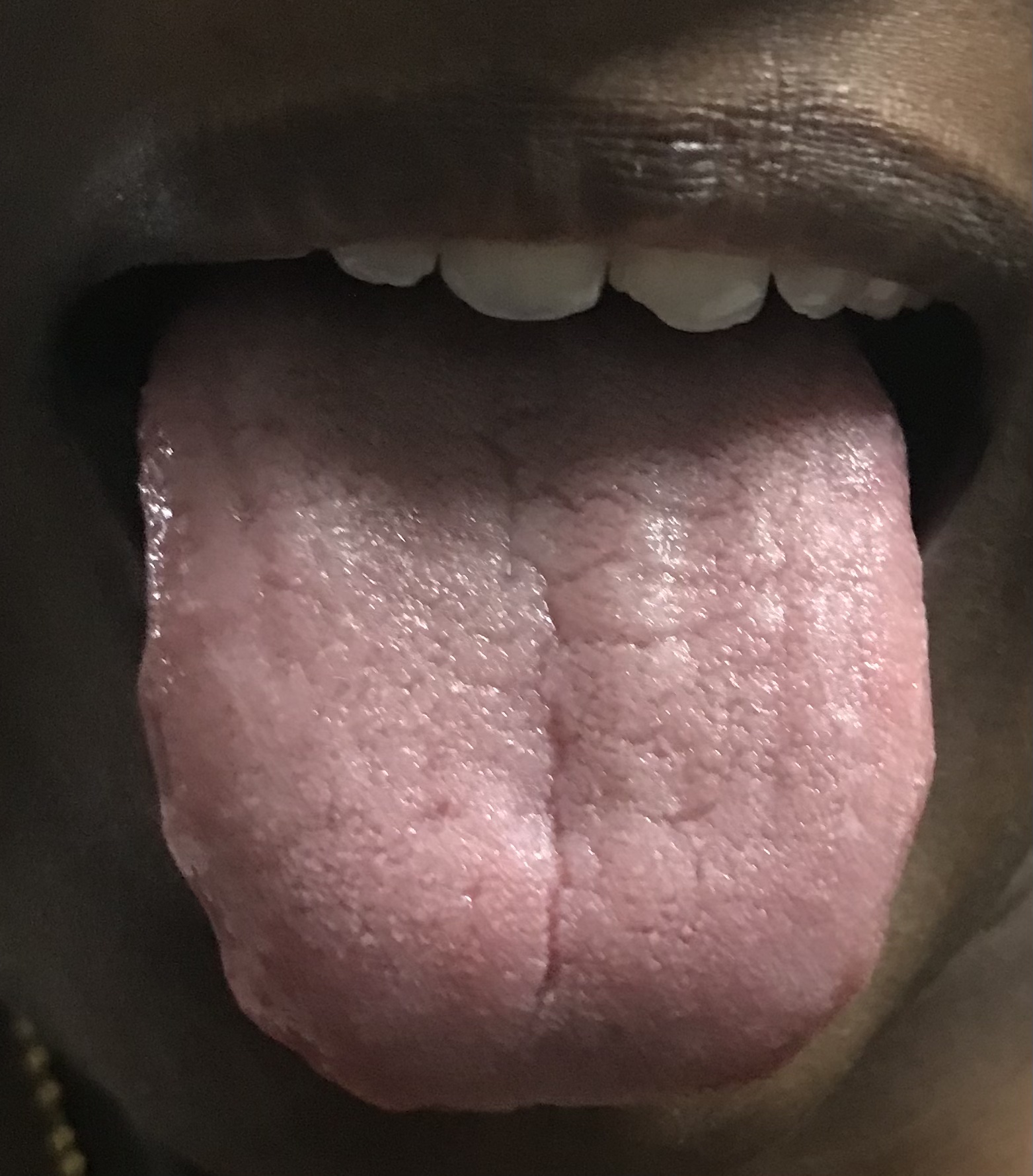
During which she noticed a left sided parotid swelling and referred to dental department and the swelling got subsided in 2 days and she complained of dryness of mouth so they took lower lip biopsy then later she developed dryness of eyes with burning sensation and dry skin with no itching.
March 2023 :
She came for follow up and referred to ophthalmology and orthopaedic department and further treatment is given .
Present complaints :
Body pains , stiffness and difficulty in walking and difficulty in getting up from the bed and needs support .
No H/o fever , cough , tingling , numbness , discolouration of skin, dental caries.
PAST HISTORY :
Not a known case of hypertension, Diabetes , TB , asthma , epilepsy , coronary artery disease .
TREATMENT HISTORY:
She was on anti rheumatoid drugs for 3 years
On Potassium syrup from 3 years (POTKLOR)
FAMILY HISTORY :
No significant family history
PERSONAL HISTORY :
She was a daily wage labourer but she stopped working since 3 years due to her illness .
Appetite: normal
Diet : mixed
Bowel and bladder : regular
Sleep : adequate
Addictions : no addictions
GENERAL PHYSICAL EXAMINATION :
Patient is conscious, coherent, cooperative and well oriented to time , place and person
Moderately built and nourished
No signs of pallor , icterus , cyanosis ,clubbing , edema , generalised lymphadenopathy.



VITALS:
Temperature: afebrile
Blood pressure :110/70 mmhg
Pulse rate : 88 bpm
Respiratory rate : 17cpm
GAIT VIDEO :
https://youtube.com/shorts/V1NxKaQvXns?feature=share
SYSTEMIC EXAMINATION:
CVS :
No visible pulsations, scars, engorged veins.
No rise in jvp
Apex beat is felt at 5 Intercostal space medial to mid clavicular line.
S1 S2 heard . No murmurs.
RESPIRATORY SYSTEM:
Shape of chest is elliptical, b/l symmetrical.
Trachea is central. Expansion of chest is symmetrical
Bilateral Airway Entry - positive
Normal vesicular breath sounds
CNS:
Sensory system - intact
Motor system - intact
Power - less
No focal neurological deficits
Speech - normal
PER ABDOMEN :
On inspection - abdomen is flat & symmetrical
Umbilicus is central and inverted
No scars, sinuses & engorged veins seen.
All 9 regions of abdomen are equally moving with respiration
On palpation - abdomen is soft and non tender
On percussion - no shifting dullness, no fluid thrill
On auscultation - normal bowel sounds are heard
PROVISIONAL DIAGNOSIS:
Sjögren’s syndrome with
Rheumatoid arthritis
Recurrent hypokalaemic paralysis 2* to distal renal tubular acidosis
INVESTIGATIONS :
- February 1 st 2023
Serum electrolytes
Sodium:142 mmol / lit
Potassium: 1.8 mmol/lit
Chloride:108 mmol/ lit
Serum calcium:9.8 mg / dl
Serum creatinine:1.3 mg/ dl
Blood urea:29 mg / dl
Urinary calcium:3.0 mg/day
Spot urine sodium:60
Spot urinary potassium:12.0
- March 13 th 2023
Hb:9.6g/dl
ESR:30mm/hr
Serum creatinine:1.1mg/dl
Serum potassium:4mmol/L
SGOT:23IU/L
SGPT:16IU/L
- March 15 th 2023
ESR:36mm/hr
Serum sodium:139mmol/L
Serum potassium:3.06mmol/L
Serum chloride:114mmol/L
Complement C3:114mg/dl (90-180mg/dl normal)
Complement C4 :63mg/dl (10-40 mg/dl normal)
Serum creatinine:0.99mg/dl
SGOT: 15IU/L
SGPT:11IU/L
BIOPSY REPORT :
Histopathological Findings: H and E stained section shows the presence of multiples lobules of minor salivary gland tissue consisting of normal appearing mucous acini with intralobular and interlobar ducts. The salivary gland tissue also shows the presence of multiple foci (25) of lymphocytic infiltrate, endothelial lined blood vessels and hemorrhagic areas Correlating with clinical features, the above histopathological features are suggestive of sjogren’s syndrome




TREATMENT:
Tab NODOSIS
Syrup POTKLOR 15ml po/TID
TAB PREGABA M 75mg po
Tab PANTOP
Tab HCQ 200mg
Tab PREDNISOLONE





Comments
Post a Comment