45 YEAR OLD FEMALE WITH VOMITINGS
THIS IS AN ONLINE E LOGBOOK TO DISCUSS OUR PATIENT'S DE-IDENTIFIED HEALTH DATA SHARED AFTER TAKING HIS / HER /GUARDIAN'S SIGNED INFORMED CONSENT. HERE WE DISCUSS OUR INDIVIDUAL PATIENT'S PROBLEMS THROUGH A SERIES OF INPUTS FROM THE AVAILABLE GLOBAL ONLINE COMMUNITY OF EXPERTS WITH AN AIM TO SOLVE THOSE CLINICAL PROBLEMS WITH COLLECTIVE CURRENT BEST EVIDENCE-BASED INPUT .
CHIEF COMPLAINTS:
A 45 yr old female who is a housewife and resident of Nagarjuna sagar came to OPD with chief complaints of nausea and vomiting since 2days , heavy menstrual bleeding since 1 1/2 yr.
HOPI:
Patient was apparently asymptomatic 2 days ago then she developed vomiting which is bilious in nature, preceded by nausea,food as its content, aggravated on taking food and water,10 to 15 episodes per day and not relieved on medication.
she also has heavy menstrual bleeding associated with clots [7/20;4 pads per day].Not associated with pain. She went to a local RMP.The symptoms have subsided for a month.Then she had same complaints within a month.
She also has a history of weight loss.She lost around 14 kgs [she was 46kgs kgs one year back and now she is 32kgs].
She also developed right ear discharge 12yrs back which is insidious in onset, intermittent in nature, mucoid and profuse discharge. Relieved temporarily on medication.H/o ringing sensation in right ear.H/o postnasal drip.She also has deviated nasal septum towards left.
She also has H/o blurred vision since 1 1/2 yr.
No H/o fever, pain abdomen, loose stools
MENSTRUAL HISTORY:
LMP: 13/07/22
Menarche at 14 yrs
Past cycles: 4/30[regular],no pain and clots,1 to 2 pads per day
Present cycles:Heavy menstrual bleeding a/w clots, no pain , 7/20,4 pads per day.
PAST HISTORY:
K/C/O DM since 13 yrs. On medication since then [Glimiperide].On insulin since 3 days
H/o Tubectomy 20 yrs ago
Not a k/c/o HTN,asthma,epilepsy,CAD
PERSONAL HISTORY:
Appetite - Normal
Diet- Vegetarians
Sleep- Adequate
B&B- Regular
Addictions - Nil
TREATMENT HISTORY:
On OHA [Glimiperide], on insulin since 3 days
FAMILY HISTORY:
Father is a k/c/o diabetes.
GENERAL EXAMINATION:
Patient is conscious ,coherent and cooperative and well oriented to time, place and person.
Ill built and malnourished.
Vitals:
Temperature - 98.4 F
PR :- 80 bpm
RR :-18 cpm
BP :- 120/60 mm Hg
SPO2 :- 95%
GRBS :- 189 mg / dl
Pallor- Present
No icterus, cyanosis, clubbing, No Generalised lymphadenopathyo, No b/l pedal edema.









SYSTEMIC EXAMINATION:
CVS-S1, S2 heard,no murmurs
Respiratory System:-
BAE- present
NVBS- heard
Per abdomen:-
soft , non tender.
CNS- NAD
EAR DISCHARGE:



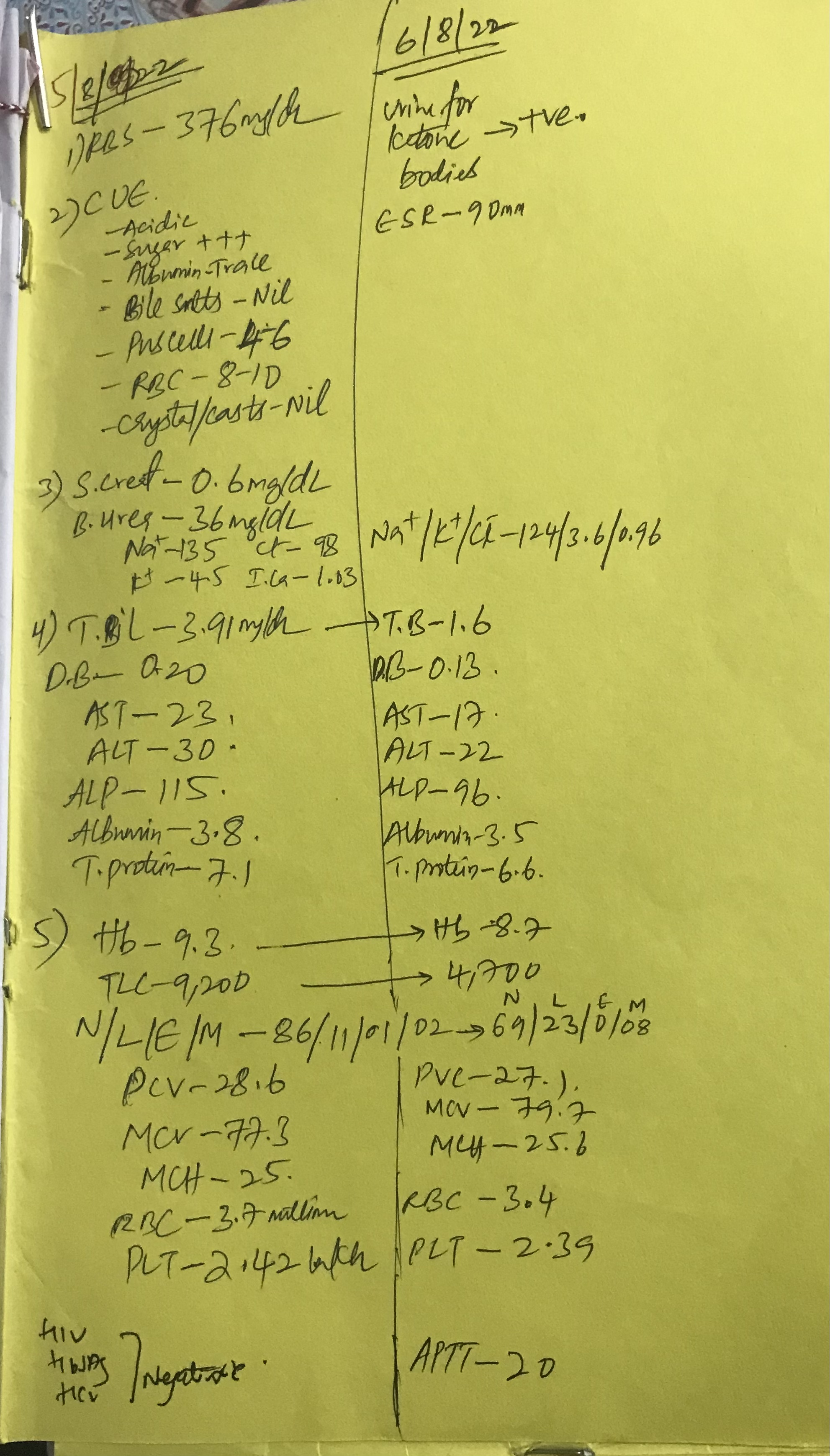
INVESTIGATIONS:

CBP ON 7/8/22





TREATMENT:
I.V fluids NS @ 100ml/hr
Inj. PAN 40mg/iv/od
Inj. Zofer 4mg /iv/tid
Insulin
Inj.5% dextrose @ 100 ml/ hr if GRBS < 200 mg/ dl
PROVISIONAL DIAGNOSIS:
DKA 2° to inadequate insulin
Adenomyosis
Anaemia under Evaluation
Type 2 DM since 13 years.

Comments
Post a Comment