48 years old male with complaints of shortness of breath and associated symptoms
CASE HISTORY:
48 year old male toddy tree climber by occupation from past 30 years . patient presented on 12/2/22 to the hospital with complaints of shortness of breath , chest pain due to cough.
HOPI:
patient was apparently 4 days back then he developed high grade fever associated with chills , rigors and relived with medication .
ASSOCIATED SYMPTOMS:
dry cough more at nights , SOB due to excessive cough.
1 episode of vomiting associated with food particles 1 day back - non bilious, non projectile, non blood stained.
Pt had similar complaints of fever associated chills and rigor in the past since 5 years
4 years back pt got hospitalized with fever and chills and got diagnosed with DM , on OHA ( metformin hydrogenchloride ) - skips medication due to alcohol abuse.
In past 5 years , pt had 5 - 6 hospital admissions with similar complaints due to heavy drinking and got diagnosed with fatty liver and jaundice.
H/o seizures since 5 years
4 - 5 episodes in last 5 years , with gap of 1 year in between the episodes .
Last episode - 1 year back
Tongue bite + , Remains in unconscious state for 5 mins
H/o multiple RTA s with minor injuries over left hand, left knee, right eye, right ankle
H/o covid + 1 year back
Received 1 dose of vaccine - covishield
PAST HISTORY:
Not a know case of hypertension ; tuberculosis; coronary artery disease; asthma
FAMILY HISTORY:
father and mother are know case of diabetes
PERSONAL HISTORY:
diet - mixed
appetite - decreased
bowel and bladder - regular
sleep - adequate
addictions -Chronic alcoholic since past 30 years
Heavy drinking since past 10 years ( 360 - 480 ml/day )
Pt went to rehabilitation for 1 year ,but never stopped drinking, as told by patient attenders , skips medications when he is on alcohol.
no know allergies to any drugs and food GENERAL EXAMINATION:
patient is conscious, coherent and cooperative well oriented to time place and person
PALLOR - ABSENT
ICTERUS - PRESENT
CLUBBING - ABSENT
CYANOSIS - ABSENT
LYMPHADENOPATHY - ABSENT
EDEMA - ABSENT



VITALS:
temp - afebrile
pulse rate - 80bpm
respiratory rate - 26cpm
spo2 - 90 %
SYSTEMIC EXAMINATION :
CARDIOVASCULAR SYSTEM :
S1 and S2 heard, no murmurs heard
RESPIRATORY SYSTEM :
Bilateral air entry present , reduced breath sounds in left IAA , IMA, ISA , on auscultation wheeze +
CNS : NAD
PA : soft, non tender

INVESTIGATAIONS:





RFT



Repeat x ray 15/2/22 :

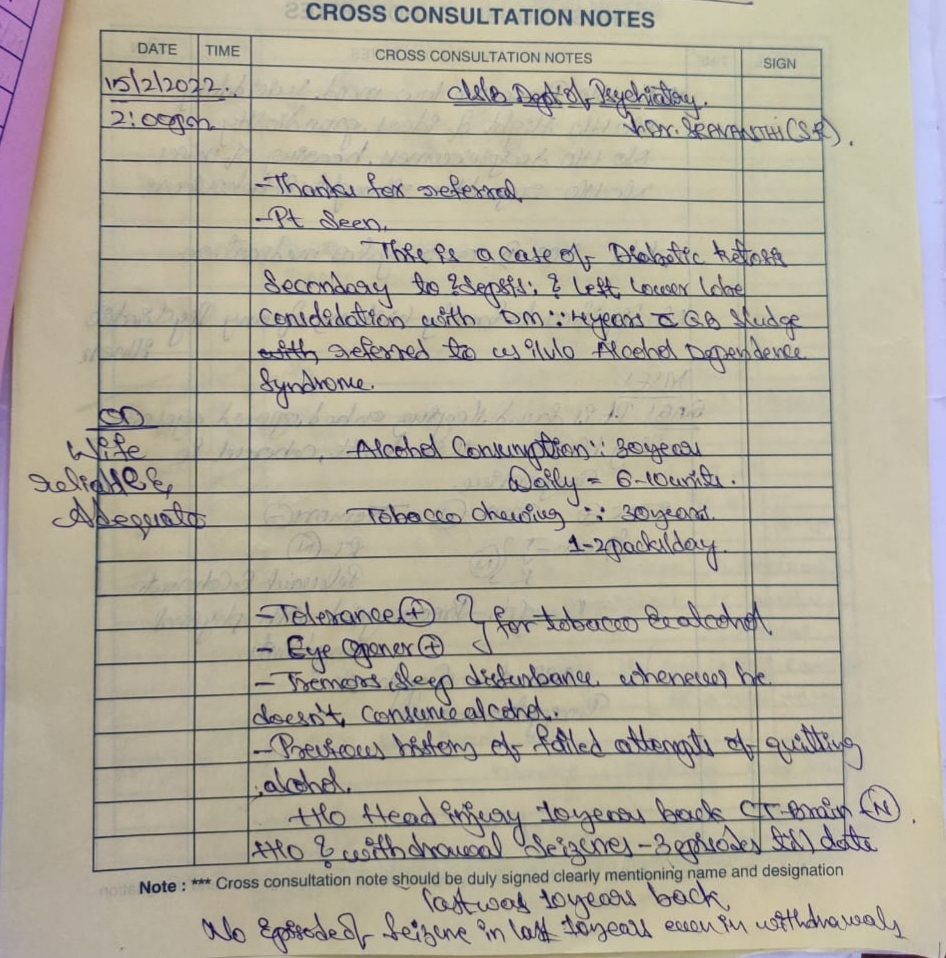
Psychiatry referral done on 15/2/22 :


17/2/22 :













PROVISIONAL DIAGNOSIS:
Diabetic ketosis ( resolved ) secondary to sepsis
Left Lower lobe consolidation
With cholelithiasis
With DM since 4 years
With Alcohol dependence
TREATMENT:
- IVF NS , RL @ 75 ml/hr
8 am 2 pm 8pm
- Inj. HAI 8 U - 8 U
NPH 10 U 10 U 10 U
- Inj. PAN 40 mg/iv/bd
- Inj. Zofer 4mg /iv/tid
- Tab. Cetrizine 5mg /Po/BD
- Tab. TusQ D capsule
- Inj. Thiamine in 100 ml NS/iv/tid
- Syp. Benadryl 5ml PO/TID
- Inj. PCM 1g /iv/sos
- Hourly GRBS charting.
- Syp. Cremaffin 30 ml/po/HS
- Inj. KCL 2 amp in 500 ml /HS/IV over 5 hrs
- Tab. PCM 650 mg/po/TID x 3 days
- Tab. Naproxen 250 mg /po/ BD x 3days

{kind=link}
Comments
Post a Comment